心源性休克
时间就是一切

随时可能发生[1]

心源性休克是种高死亡率疾病,需要针对性的治疗来改善血流动力学紊乱[2]
设计治疗方案
识别
任何改善 CS 结果的尝试都应该从早期识别开始。包括具有早期识别和个体化治疗能力的多学科 CS 团队医疗模式。[3]
启动
专家建议使用高级血流动力学监测来诊断和/或管理 CS 患者。[4]为了避免正性肌力药的负面影响,应考虑尽早启动主动脉内球囊反搏。[5],[6]
评估
需要结合患者状态和血流动力学的快速反馈循环来评估对初始治疗的反应。[2]
升级
当患者对治疗没有反应时,如果需要的话,可以考虑下一阶段的支持并转移到经验丰富的休克治疗中心。[4]
识别至关重要
心源性休克阶段 [4]
风险期:具有心源性休克危险因素,但目前没有症状或体征的患者。例如,大面积急性心肌梗死,既往心肌梗死,急性和/或急慢性心力衰竭。
开始期:患者有相对低血压或心动过速的临床证据,但没有灌注不足。
典型期:患者表现为灌注不足,需要进行容量复苏以外的干预(正性肌力药、升压药或机械支持)。这些患者通常表现为相对低血压。
恶化期:患者对最初的干预措施没有反应。类似于典型期阶段,而且越来越糟。
终末期:患者需接受多种干预,可能在进行心肺复苏时出现心脏骤停。
任何改善心源性休克结果的尝试都应该从早期识别开始。包括具有早期识别和个体化治疗能力的多学科团队医疗模式。[3]
早期启动
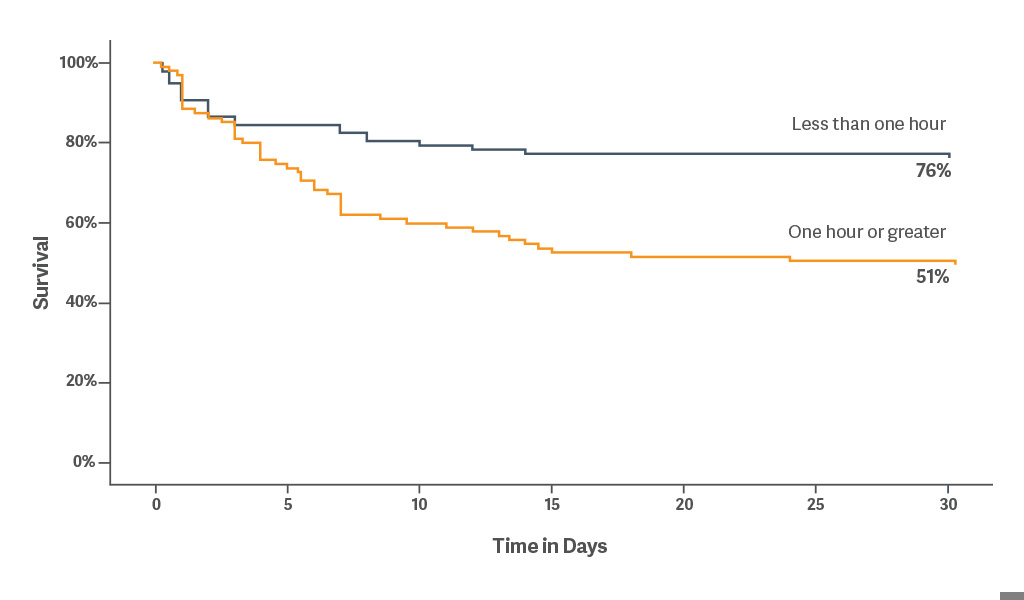
回顾性分析表明,早期使用机械循环支持 (MCS) 是一种重要的治疗干预措施。无论病因如何,尽早使用主动脉内球囊反搏都会带来生存获益。[5]
当 IABP 在心源性休克发生 1 小时内放置时,30 天生存率为 76%。[5]
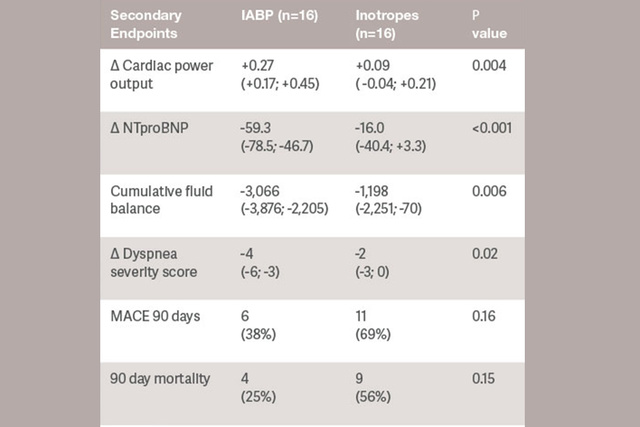
尽早使用 IABP 稳定血流动力学可作为晚期失代偿性心力衰竭的主要治疗手段。[6]
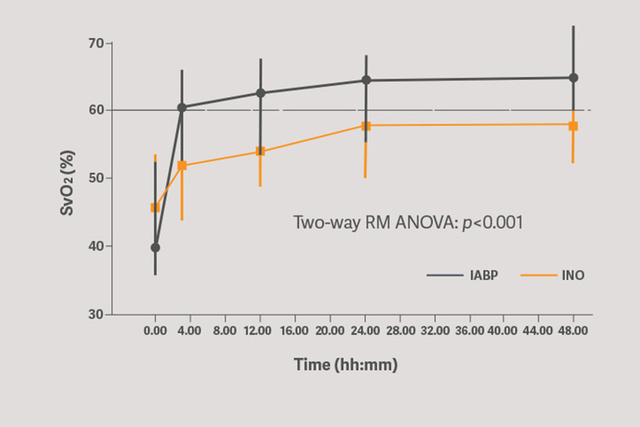
SVO2 评估结果表明,采用 Sensation Plus 50 cc IABP 的主要循环支持能够显著改善器官灌注。[6]
启动支持可立即减少每搏做功,可能会降低心肌耗氧量。IABP 反搏疗法可降低 LV 后负荷、前负荷和心室内不同步性。[6]
为了避免血管活性药物的负面影响,应考虑尽早启动 IABP 治疗。[5],[6]
评估有效性
为患者量身定制护理服务,并根据需要进行升级。评估治疗反应对于调整护理方案至关重要。[2]
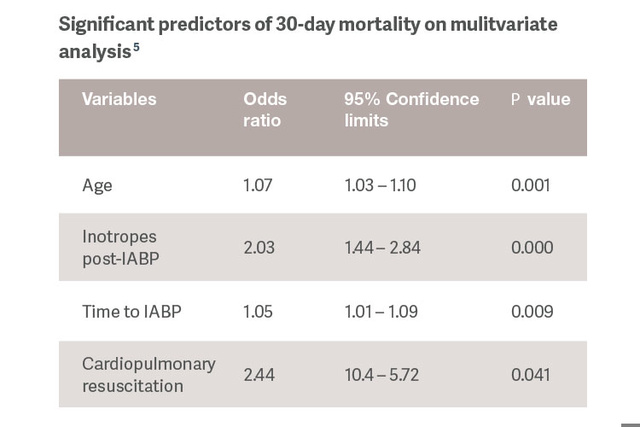
识别对 IABP 支持的反应的预测指标,使能够为患者量身定制治疗方案,并为 CS 晚期阶段的患者备用更强大的 MCS 设备。[5]
IABP:安全的一线 MCS 治疗方案
| 物品 | 患者人数 | 死亡率 | 出血 | 中风 | 血管 并发症 |
AKI |
| Dhruva 2019[8] | 1680 来自 NCDR 的成对匹配 * |
支持 IAB 绝对 差值 10.9% |
支持 IAB 绝对 差值 15.4% |
NA | NA | NA |
| Amin 2019[9] | 48306 Premier 数据库* |
支持 IAB p < 0.0001 |
支持 IAB p < 0.045 |
支持 IAB p < 0.0001 |
NA | 支持 IAB p < 0.052 |
| Wernly 2019[10] | 588 4 项 RCT 的 Meta 分析 ** |
无差异 p = 0.38 |
支持 IAB p < 0.002 |
无差异 p = 1.00 |
支持 IAB p < 0.01 |
NA |
| Schrage 2011[11] | 237 来自 IABP-Shock II 的成对匹配 ** |
无差异 p = 0.64 |
支持 IAB p < 0.01 |
NA | 支持 IAB p < 0.01 |
NA |
并发症问题
IABP 不会增加出血
| 试验 | IABP | 无 IABP |
P 值 |
| CRISP AMI:大出血 [12] | 3.1% | 1.7% | 0.49 |
| CRISP AMI:主要血管 [12] | 4.3% | 1.1% | 0.09 |
| SHOCK II:中度出血 [13] | 17.3% | 16..4% | 0.77 |
| SHOCK II:大出血 [13] | 3.3% | 4.4% | 0.51 |
| SHOCK II:主要血管 [13] | 4.3% | 3.4% | 0.53 |
试验登记:CRISP AMI,n = 337;SHOCK II,n = 600
IABP 疗法仍然是主要的 MCS 设备,是值得信赖、有价值的主要治疗方案 [8], [9], [14]