
急性呼吸窘迫综合征 (ARDS) 的识别与优化治疗
急性呼吸窘迫综合征(ARDS)是一种认识不足、治疗不足、死亡率高的综合症。急性呼吸窘迫综合征(ARDS)的早期治疗是一个渐进式的窗口[1]
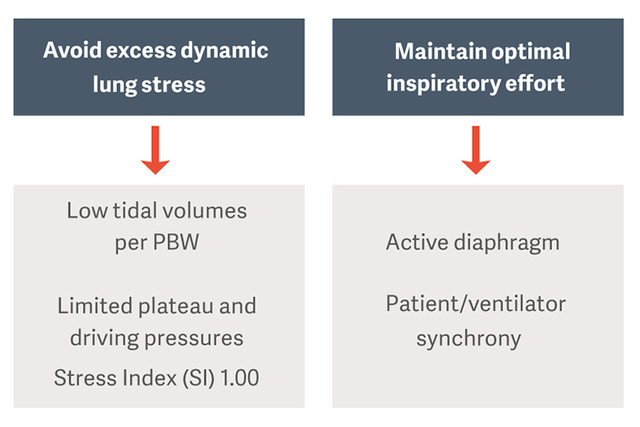
如何预防过度的动态肺应力和膈肌损伤?

78% 的 ARDS 患者在有创通气的前 48 小时发生。

82% 的患者得到小于 12cmH2O 的 PEEP
35% 的患者得到的潮气量超过 8ml/kg 理想体重。
23-84% 患者遭受隔肌受损与不良的结果。
见参考文献 [1]
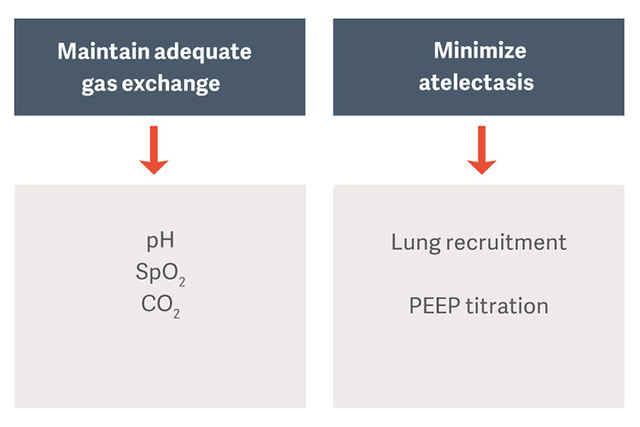
肺和隔肌保护性通气
ARDS 患者机械通气的目的是维持气体交换,同时避免呼吸机诱导的肺损伤 (VILI)、呼吸机相关性肺炎 (VAP) 或呼吸机诱导的膈肌功能障碍 (VIDD) 等并发症。[2]
什么是驱动压力?
驱动压力(ΔP)是肺应变的间接测量。它被定义为总呼吸系统顺应性(ΔP=VT/CRS)的潮气量之比,并且可以对没有进行吸气努力的患者进行常规计算,如平台压力减去PEEP(ΔP=Pplateau-PEEP)。
Amato 等人认为 ΔP 是呼吸机诱发性肺损伤(VILI)的主要决定因素,并且呼吸机参数与死亡率密切相关,特别是在 ΔP 值> 14 cm H2O 时 [1][3]。将 ΔP 作为减少肺损伤的目标是改善患者术后效果的合理方法。

保护性潮气量 6 ml/kg PBW
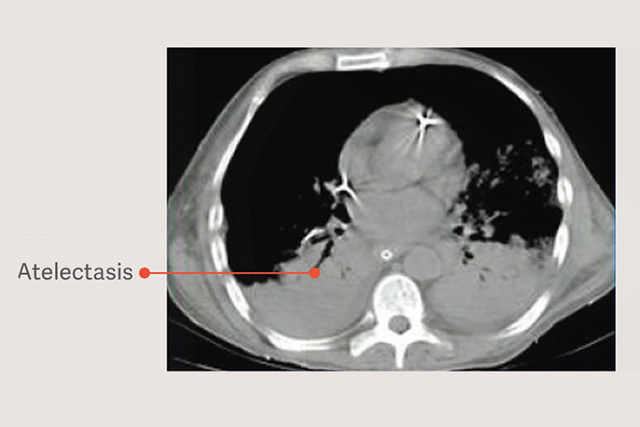
ARDS 患者有依赖性肺不张,这种肺不张在机械通气过程中会因减少可用于潮气通气的肺体积和增加肺压力而加重肺损伤,即使在使用“安全”潮气量时也是如此。[6]
")
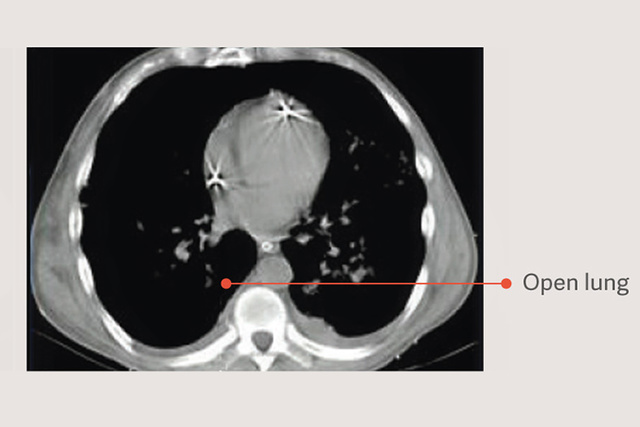
开放肺方法 (OLA)
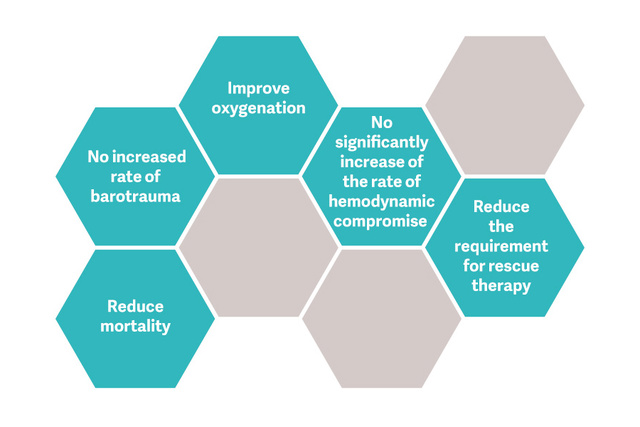
开放肺法(OLA),包括肺复张通气策略和PEEP滴定,会显着改善氧合,同时减少肺部损伤。[2] [6] 在 OLA 试验中,氧合和驱动压力都得到了改善,不会对死亡率、撤机天数或气压伤产生不利影响 [7]。这项试验还显示了 ARDS 患者死亡率极低的报告之一:25%。
图形参考 [7]
肺复张通气策略(RM)是否具有价值?
肺复张通气策略(RM)是否具有价值?
保持卓越的吸气效果并保护隔肌

为什么要保护隔肌?
隔肌无力在 ICU 患者中普遍存在 (23-84%),并始终与预后不良相关 [12]。 29% 的患者由于膈肌功能障碍而经历撤机失败,并将机械通气时间延长至 16 天 [13]。
Edi 监测
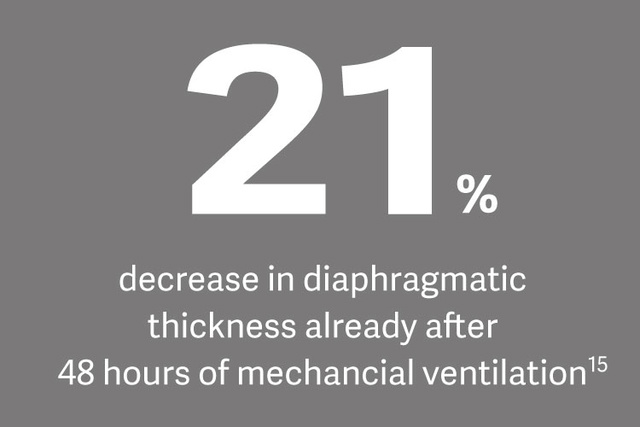
防止废用性萎缩和高呼吸强度是膈肌保护性机械通气的基础,Edi 监测被认为是一种针对膈肌生理负荷的方法。[14]
临床上的影响
Ewan Goligher 博士根据新的一项主题研究表示,膈肌无力的存在显著增加了撤机困难、撤机时间延长和住院死亡率的风险。